OCD of the Distal Intermediate Ridge of the Tibia
What is OCD of the distal intermediate ridge of the tibia?
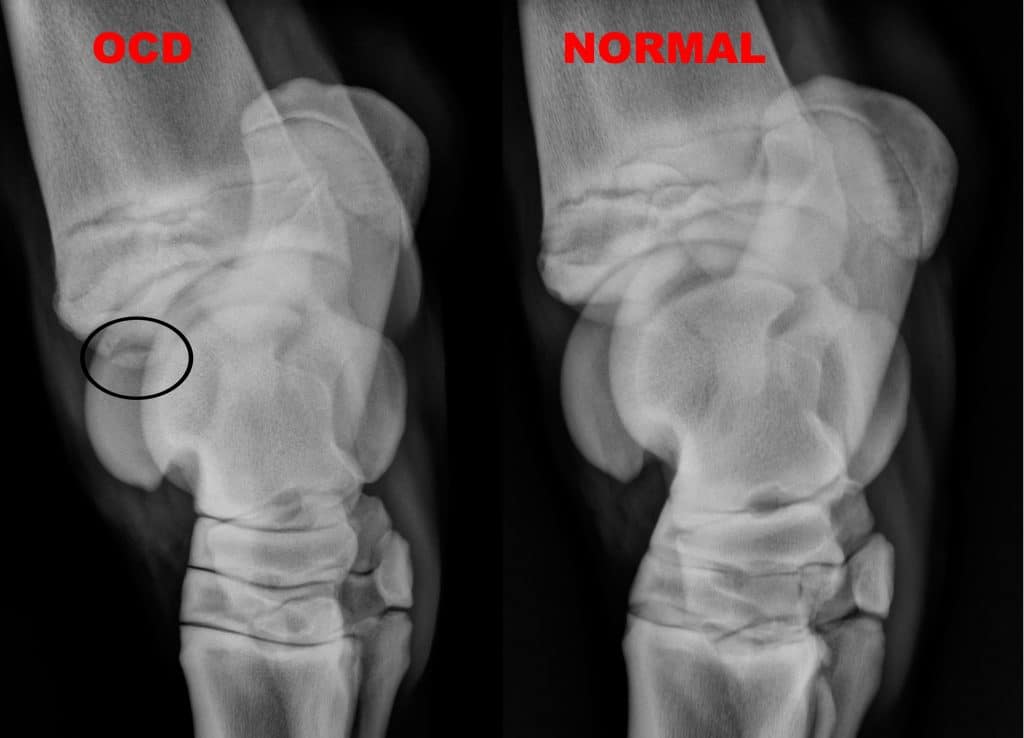
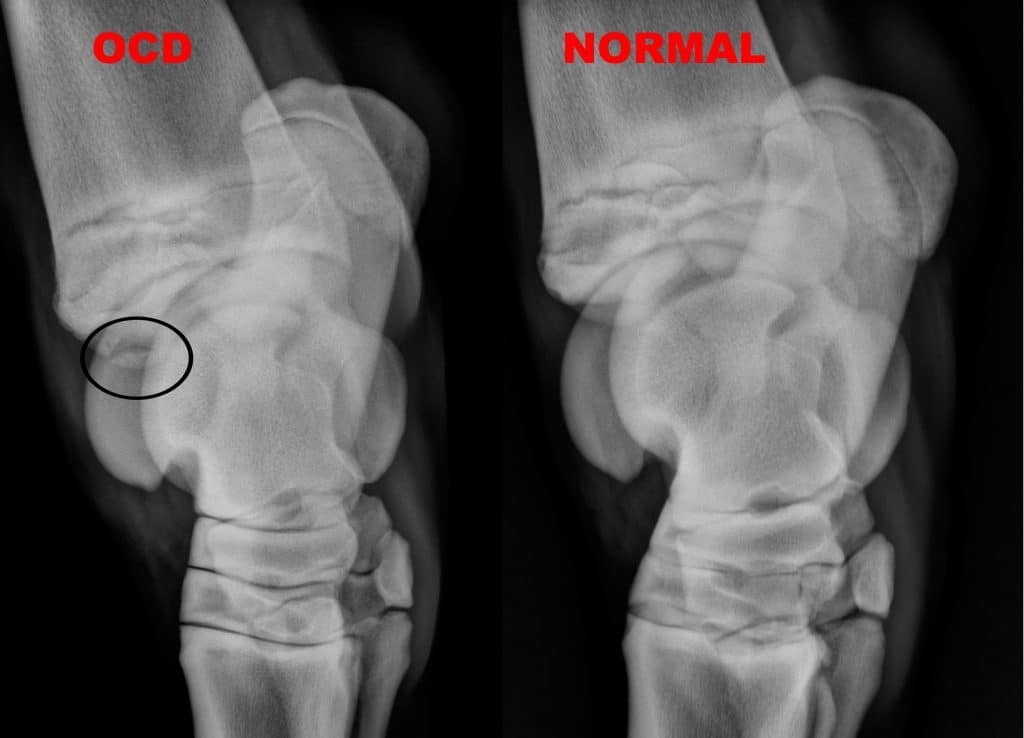
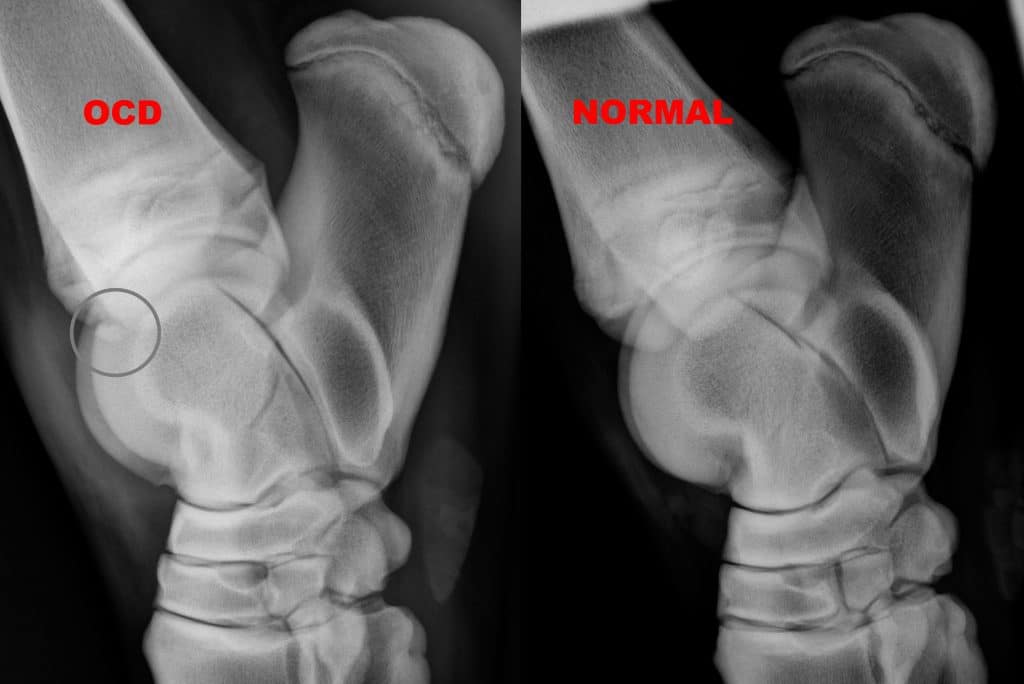
The most common joint in which to diagnose osteochondritis dissecans (OCD) in the horse is the tarsus. The most common location for OCD is the cranial distal aspect of the intermediate ridge of the tibia. This type of OCD appears as a bony fragment in the area of the intermediate ridge of the tibia. The bone fragments remain loosely attached to the bone of origin, but debris and inflammatory enzymes are released into the joint from under the fragments that result in synovitis or joint inflammation.
What is OCD?
Although the exact cause of OCD and the steps leading up to it are not definitively known, there is a reasonable consensus about the general cause. Failure of the developmental process leads to a disturbance in the formation of joint cartilage and the bone supporting it. The resultant cartilage and subchondral bone is irregular in thickness and weaker than in normally developing areas. Forces placed on these abnormal areas when the horse ambulates may cause further damage to the abnormal tissue. This can lead to several problems which are recognized as OCD, including local detachment and fracture of cartilage and bone. These detached areas may remain partially attached to the surrounding tissue, which then exist as loose flaps of tissue, or may become completely detached, resulting in free-floating islands which can travel throughout the joint. These loose flaps and islands of abnormal cartilage and bone can cause inflammation in the joint, and over time may cause damage to the normal cartilage.
Causes and Risk Factors
Several causes of OCD are known, although the disease is generally considered to be multifactorial. As a result, the disease is not usually caused by any one factor, but rather a combination of several factors acting together.
These known factors include:
Rapid growth and large body size: An unusually rapid phase of growth and/or growth to a large size can be associated with OCD formation.
Nutrition: Diets that are very high in energy or have an imbalance in trace minerals, low-copper diets in particular, can lead to OCD formation.
Genetics: Risk of OCD may also be partially inherited, although the mode of inheritance is not well defined and other factors are often required before an OCD fragment forms. Genetics can also be responsible for the horse’s response to the other factors presented here, as well as rate of body growth.
Hormonal imbalances: Imbalance in certain hormones during development, including insulin and thyroid hormones, can encourage OCD formation.
Trauma and exercise: Trauma to a joint, including routine exercise, is often involved in formation and loosening of the OCD flap or fragment.
Clinical findings with OCD of the intermediate ridge of the tibia:
The most common clinical finding is effusion (swelling within the joint) of the tibial tarsal joint (Bog Spavin). If there are multiple or large fragments of bone present, clinical signs may also include a variable degree of lameness in addition to the effusion. Many horses with OCD of the intermediate ridge of the tibia are asymptomatic even though fragments of bone are seen in the purchase exam radiographs. Bilateral involvement (both hock joints) is sufficiently common that the opposite joint should always be radiographed. The signs of hock OCD are usually first seen in non-racehorses just prior to or at the beginning of training.
Diagnosis of OCD of the intermediate ridge of the tibia:
Radiographs (X-rays) of the hocks are the diagnostic modality of choice for diagnosing this disease.

Treatment of OCD of the intermediate ridge of the tibia:
Although lameness is usually minimal with this type of OCD, surgery is the recommended treatment. Surgery should be considered early enough in the course of the disease so that the joint capsule is not unduly stretched making resolution of the joint effusion less likely. The most common technique used for surgical removal of OCD fragments is arthroscopy. Arthroscopic removal is usually preferable to arthrotomy (an open joint approach), since skin incisions are small, less surgical trauma is caused, post-surgical recovery time may be reduced, and a more thorough exploration of the joint can be performed at the time of surgery. Arthroscopic OCD fragment removal usually requires general anesthesia. The surgeon makes two or more small incisions into the joint through which an arthroscope is placed to visualize the joint and instruments are introduced to remove the OCD fragments.
Prognosis:
When the fragments are associated with clinical signs, arthroscopic surgery for removal is very successful.